Herd Immunity: Do high rates of vaccination make us safe?

Most of us have probably heard of the “herd immunity” concept. It goes a little something like this: If 95% of the population become immune to a disease via vaccination, there will not be enough vulnerable individuals to allow the disease to spread, thus protecting the portion of the population (herd) who cannot be vaccinated (those who are too young or immunocompromised in some way).
Summary:
- Scientists developed vaccinations based on the natural herd immunity derived from pathogen exposure. The immunity derived from vaccines was theorized to be equal to natural immunity, yet superior in terms of risk of infection. For several generations this appeared to be the case. Due to new evidence, it became apparent that the vaccines had not been as effective as they thought. To cover the disparity, successively higher percentages of the population required for herd immunity to take effect have been imposed.
- New research was performed and booster shots were introduced to mimic the natural re-exposure process. In the meantime, more incidences of reported vaccine injury have led to the discovery that a much larger and unidentifiable portion of the population suffer adverse effects from vaccination in many cases equal to or much more severe than the adverse effects of the diseases they are vaccinated against.
- However, in order to maintain the high percentage of the population required to achieve herd immunity- these injuries are minimized and in many cases denied in order not to discourage the population from vaccination. All the while, they are working to usher in a “golden age” of vaccines that will be “personalized” to avoid an individual’s genetic predispositions toward certain vaccine injuries.
- Unexpected side effects of mass vaccination programs have manifested such as the “shifting” of susceptible populations (creating problems where they didn’t exist previously), absence of maternal immunity passed to infants, introduction of a “quasi-sterile” environment that is resulting in an increased susceptibility to diseases once considered “eradicated”. The latter is evidenced by the ever increasing reports of disease break outs in predominantly vaccinated populations as well as break outs in mixed populations.
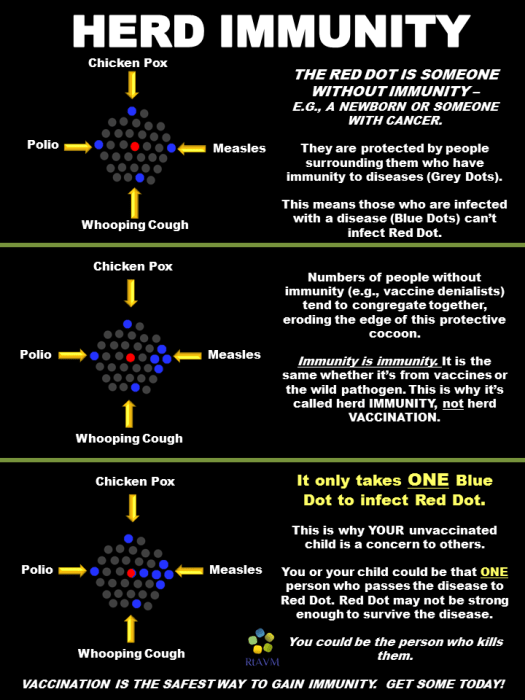
Here is a nice little vaccine propaganda diagram explaining the concept of herd immunity visually, but leaving out the important bit of information there are a group of individuals who are highly susceptible to substantial vaccine injury.
This mantra is reinforced over and over and over.
We hear it on TV. You read about it online. Medical journals publish papers about it. Newspapers write articles about it. Schools teach it. Now we are worked up into a frenzy over it and the debate is HOT on both sides because we’re talking about how the actions of others effect your well-being or the well-being of your children. People who choose not to vaccinate have become public enemy #1 because they are “threatening the nation’s herd immunity” and placing everyone’s health at risk. Honestly, people are getting down right nasty.
This unfortunate attitude is rooted in the fact that we have all been indoctrinated to a large extent to believe that the science behind the benefit of vaccinations is settled. We assume since we have been given vaccines since the late 1800’s, doctors and scientists know exactly how this process works and exactly what the outcomes will be. I for one, thought on many occasions when I was younger how lucky I was to be born into a time when science had all this “stuff figured out” so that I didn’t have to suffer from horrific preventable illnesses.
In my naivete, it never occurred to me that these mass vaccination programs were instituted prior to sufficient research- in more of a “let’s implement our educated hypothesis and see how it goes” scenario.
Case in point, the approval of a new vaccine.
The US Vaccine Advisory Panel, called the Advisory Committee on Immunization Practices (ACIP), is the group that approves vaccines for public use in the United States. Most members have connections to the pharmaceutical (aka vaccine) industry.
This 4-minute video was taken from a recent ACIP meeting discussing the approval of a new Hepatitis B vaccine for ADULTS. The vaccine uses a new ingredient that has NEVER been used before…
Pre-approval studies signaled an increase in heart attacks…but under pressure from vaccine makers, the committee unanimously APPROVES the vaccine.
Meaning…YOU ARE THE TEST SUBJECT!
But your doctor won’t tell you that…
The public has always been the under-informed guinea pig and continues to function in the same capacity today- though we are conditioned to ignore the everyday evidence of this that surfaces in the form of the massive number of reports of vaccine injury and vaccine failure. Those who are rudely awakened from the farce and begin to speak out against the status quo are ridiculed and invited to don a “tin foil” dunce cap. At this point, if you are questioning my statements regarding the “settled science” on vaccines, I hope you will read the extensive evidence I have documented in my article: 6 Things You Need to Know When Deciding Whether or Not to Vaccinate. Now, on to the topic at hand…
Does “herd immunity” exist? Absolutely!
The problem is, herd immunity through vaccination– does NOT exist. The theory of herd immunity through vaccination is based on the documented proof of the natural immunity that occurs after exposure to certain illnesses. “Safer” exposure through vaccination in place of actual exposure through natural infection, in theory, should impart the same level of immunity as the natural process affords. It’s a great theory. But have you ever heard the old saying, “If it sounds too good to be true, it probably is”? We receive a harmless vaccine, we never have to worry about getting a yucky disease. Countless lives are saved. The end. However, that’s not exactly how it has played out in the real world. Instead of “protecting the weaker members of the herd” we are merely “shifting around” the members of the herd susceptible to disease. But don’t expect to hear that in the mainstream. Let me explain.
First of all, where did we come up with the magic number of 95% vaccination as the requirement to achieve herd immunity? The idea was born in the 1930’s when Johns Hopkins University’s Arthur Hedrich discovered that after 55% of Baltimore’s population contracted measles (and subsequently became immune to measles) the rest of the population became protected. So, in November of 1966, the US Public Health Service announced a mass vaccination program aimed at vaccinating 55% of the population which would eradicate measles in the US by 1967.
The problem is- it didn’t work. Despite achieving the 55% vaccination rate, measles was not eradicated by 1967. (Our first clue that natural immunity is far superior to vaccine immunity.) So, they increased the required vaccination percentage to 70-75%. When that failed, the percentage was increased to 80%. Then 83%. Then 85%. Then 90% in 2001. Currently, we are at the number 95% and many studies are now calling for 100% required rates. (What was that about protecting those members of the herd that are not able to tolerate vaccination again?)
So was Hedrich wrong? Or is there a difference between the natural immunity derived from contracting diseases and the immunity derived from vaccinations?
Dr. Hedrich had observed that 95% of the children in cities had contracted measles by the time they reached the age of 15. Before the measles vaccine was introduced, measles outbreaks occurred cyclically every 2 to 3 years. So, 95% of the population was immune to measles by their 15th birthday. (Here’s the link to this research: https://academic.oup.com/aje/article-abstract/11/3/576/63159/THE-CORRECTED-AVERAGE-ATTACK-RATE-FROM-MEASLES)
Scientists at this time worked on the assumption that one vaccine would result in lifetime immunity. And indeed for decades we have operated under the assumption that the infectious diseases that we are vaccinated against are all but eradicated. Almost no one gets them, ergo vaccines work. Right?
Actually, for over 70 years doctors assumed that vaccine immunity was lifelong. No one vaccinated during these years received booster shots. It wasn’t until much later that it was discovered that vaccine protection only lasts from 2 to 10 years. So, the first generations to be vaccinated in childhood likely had no immunity by the time they reached adulthood. Renowned neurosurgeon, Dr. Russell Blaylock writes, “If we listen to present-day wisdom, we are all at risk of resurgent massive epidemics should the vaccination rate fall below 95%. Yet, we have all lived for at least 30 to 40 years with 50% or less of the population having vaccine protection. That is, herd immunity has not existed in this country for many decades and no resurgent epidemics have occurred.” You can read Dr. Blaylock’s vaccine herd immunity article here: http://www.vaccinationcouncil.org/2012/02/18/the-deadly-impossibility-of-herd-immunity-through-vaccination-by-dr-russell-blaylock/
Years later scientists discovered that the body is best able to defend itself due to ongoing re-exposure to pathogens. A study by A.A Navarini concluded, “The formal demonstration that both maternal antibodies and early exposure to infection are required for long term protection illustrated that constant re-infection cycles have an essential role in building a stable herd immunity.” (Here is the link to that study: https://www.ncbi.nlm.nih.gov/pubmed/19877011)
And voila! That’s how we ended up with vaccine boosters- in order to mimic natural re-exposure. But, this hasn’t exactly fixed the problem.
Navarini has also noted that vaccination creates a “quasi- sterile” environment that actually makes the population more vulnerable to disease outbreaks. “Attempts to eradicate measles virus or poliovirus eliminates antigen exposure of infants to these pathogens. Such quasi-sterile epidemiological situations may actually increase the risk of outbreaks.”
Indeed, today, several generations after these diseases were declared to be all but eradicated, we have multiple examples of outbreaks in 100% or near 100% vaccinated populations:
CDC documented case of measles outbreak in 100% vaccinated population: https://www.cdc.gov/mmwr/preview/mmwrhtml/00000359.htm
Measles outbreak traced to fully vaccinated patient: http://www.sciencemag.org/news/2014/04/measles-outbreak-traced-fully-vaccinated-patient-first-time
Mumps: https://academic.oup.com/cid/article/47/11/1458/282575/Mumps-Outbreaks-in-Vaccinated-Populations-Are
Chicken Pox: http://pediatrics.aappublications.org/content/113/3/455
Pertussis: http://www.medscape.com/viewarticle/857368
Looks like Navarini is on to something…This leaves us with the all important question: Why are we becoming more susceptible to these diseases?
Well, one of the primary differences between natural immunity and vaccine immunity is that vaccine induced immunity cannot be passed from mother to infant. Why? Because exposure through the mucous membrane is what contributes to the production of antibodies in the mammary gland. But injected vaccines bypass the mucous membranes all together and only blood antibodies are produced. So, even if the mother does have immunity through vaccination, she can’t pass it to her infant through breastfeeding like a naturally immune mother can. On the flip side of the coin however, if a mother has natural immunity, and her infant is exposed to measles- the infant will contract an asymptomatic infection (an infection with no symptoms) that will result in lifetime immunity to measles.
A study published by M. Papania in 1999 states, “Infants whose mothers were born after 1963 had a measles attack rate of 33%, compared to 12% for infants of older mothers…Infants whose mothers were born after 1963 are more susceptible to measles than are infants of older mothers. An increasing proportion of infants born in the United States may be susceptible to measles.” (Here is the link to the study: https://www.ncbi.nlm.nih.gov/pubmed/10545585)
In effect, while the measles vaccine reduced the expression of measles infections, it has had a detrimental effect when you recognize it has merely “swapped” the population groups susceptible to the disease. (Now infants, and non immune adults.)
As Dr. Suzanne Humphries notes, “Infants used to be protected by maternal antibodies, adults were protected by routine exposure, and infected children came through the disease normally with long term immunity.” (FYI: measles never was highly dangerous in the US. It is only dangerous in malnourished populations. As a matter of fact 30% of measles infections went undetected because they were so mild. This is at a stark contrast with the vaccine, which has a higher incidence of serious injury in the US than the disease itself.)
An example my generation will identify with is chicken pox. When I was a kid, everyone got chicken pox at some point. Though certainly annoying, most cases of chicken pox are pretty benign and when you recover there is a 95% natural immunity rate. However, the advent of the mass varicella vaccination program has resulted in members of the “herd” being unable to pass natural immunity to each other. Now shingles is on the rise. Shingles is MUCH worse than chicken pox.
This National Institutes of Health release documents the failure of the varicella vaccination program (yet it is still recommended- go figure), “Varicella vaccination is less effective than the natural immunity that existed in prevaccine communities. Universal varicella vaccination has not proven to be cost-effective as increased HZ morbidity has disproportionately offset cost savings associated with reductions in varicella disease. Universal varicella vaccination has failed to provide long-term protection from VZV disease.”
Dr. Goldman of the above varicella study, notes in this separate document (http://www.vaccinationcouncil.org/wp-content/uploads/2012/07/Goldman-SummaryofChickenpoxVaccine1.pdf) that the varicella vaccination program has had the effect of “shifting chickenpox to a more vulnerable adult population where chicken pox carries 20 times more risk of death and 15 times more risk of hospitalization compared to children. Add to this the adverse effects of both the chicken pox and shingles vaccines as well as the potential for increased risk of shingles for an estimated 30 to 50 years among adults.” In simple terms: we were better off before the vaccine.
Now, the theoretical vast good that vaccinations could do has been greatly diminished due to the fact that the vaccines in and of themselves are dangerous and in many cases carry a much higher risk of injury than the illnesses they are designed to prevent. The unexpected problem has been, however, that a far larger portion of the population are susceptible to adverse vaccine effects on a varying scale of severity. Vaccine injury encompasses a plethora of complications not currently recognized in their full scale which leads to massive under-reporting of vaccine side effects.
The medical and science fields (quietly) admit that a much larger portion of the population than originally expected are susceptible to vaccine injury.
They also confirm that currently, there is no way to reliably determine who these individuals are. Of course this is not discussed in the mainstream, but here is the link “to the next golden age in vaccinology to be ushered in by the new science of vaccinomics”: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2831634/ . The very existence of this document speaks the truth that they are aware that vaccines cannot be safely administered in their current “one size fits all” form, but they won’t let us know that until they have the new and improved product ready to fill the void. The linked document is all about the up and coming “personalized” vaccines that they tell us will be safer. (Safer than our already extremely “safe” vaccines?) Here’s another quote from the article, “In addition, newly available data suggest that some vaccine-related adverse events may also be genetically determined and, therefore, predictable.”
The medical and science communities answer by once again calling for higher vaccine rates and introducing new vaccines by the truckload.
Every Child By Two is a front group for vaccine makers, the primary source of their funding. Don’t take my word for it, the prestigious British Medical Journal ran an expose of many groups like Every Child By Two titled, “The unofficial vaccine educators: are CDC funded non-profits sufficiently independent?”
Herd Immunity the Marketing Gimmick: JB Handley
Additional sources: http://www.vaccinationcouncil.org/2012/07/05/herd-immunity-the-flawed-science-and-failures-of-mass-vaccination-suzanne-humphries-md-3/



